Les valvulopathies aortiques sévères peuvent s’accompagner de signes d’hypertrophie/dilatation ventriculaire ou atriale gauche non spécifiques. Des anomalies de conduction sur la branche gauche sont fréquentes.
NB. L’ECG n’est pas un outil précis pour apprécier la sévérité d’une valvulopathie aortique. L’intelligence artificielle semble utile [3].
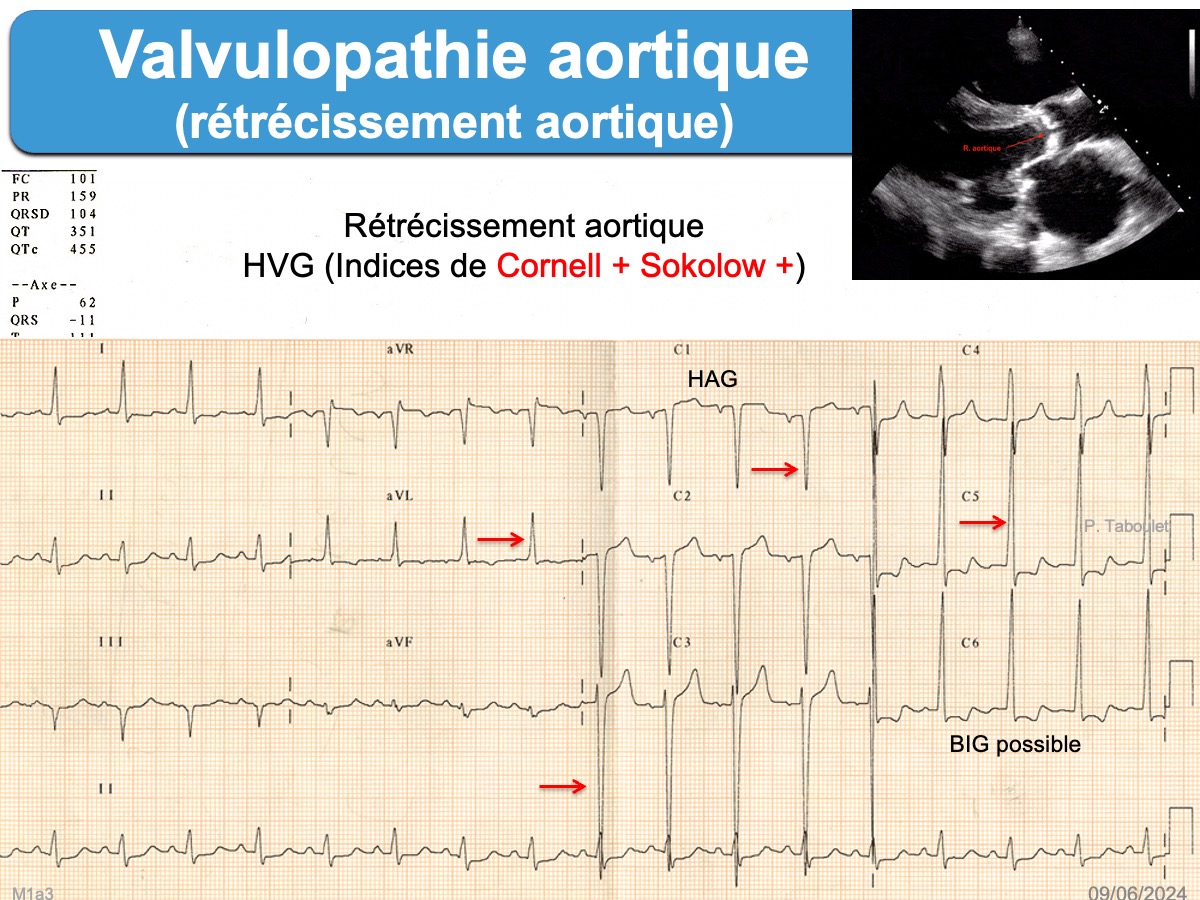
Rétrécissement aortique
Les signes ECG associés sont :
- hypertrophie atriale gauche
- hypertrophie ventriculaire gauche (parfois gigantesque, de type systolique avec T < 0 en précordiales gauches)
- bloc incomplet gauche, bloc de branche gauche ou simple déviation axiale gauche
- Le strain pattern (repolarisation de type « surcharge ventriculaire ») est un signe de sévérité de l’hypertrophie, de mauvais pronostic [1][2]
- L’ECG peut être normal
Une maladie des coronaires est fréquemment associée aux formes calcifiées.
Insuffisance aortique
Les signes ECG associés sont : hypertrophie atriale gauche et hypertrophie ventriculaire gauche, parfois de type diastolique (avec ondes T positives en précordiales gauches). L’hypertrophie VG peut être particulièrement sévère et s’accompagner d’ondes q de pseudo nécrose au niveau des dérivations où l’onde R est proéminente. Le strain pattern est un signe de sévérité, de mauvais pronostic.

Si vous souhaitez améliorer ce contenu, merci de me contacter
Livre ECG de A à Z et autres (P. Taboulet, 2e ed. 2025)
Faites des quiz sur le site web (plusieurs niveaux de connaissance 1 à 3).
YouTube : ma playlist https://www.youtube.com/c/PierreTaboulet-ECG)
YouTube : ECG Minute (hebdomadaire 10 min)
Inscrivez-vous à ma newsletter hebdomadaire (https://www.e-cardiogram.com/newsletter)
[1] Greve AM, Boman K, Gohlke-Baerwolf C, et al. Clinical implications of electrocardiographic left ventricular strain and hypertrophy in asymptomatic patients with aortic stenosis: the Simvastatin and Ezetimibe in Aortic Stenosis study. Circulation. 2012;125(2):346-53 (téléchargeable)
The predictive value of ECG left ventricular strain (defined as T-wave inversion in leads V4 through V6) and LVH, assessed by Sokolow-Lyon voltage criteria (RV5–6+SV1 ≥35 mV) and Cornell voltage-duration criteria {[RaVL+SV3+(6 mV in women)]×QRS duration ≥2440 mV · ms}, was evaluated by adjustment for other prognostic covariates. A total of 1533 patients were followed for 4.3±0.8 years (6592 patient-years of follow-up), and 627 cardiovascular events occurred. ECG strain was present in 340 patients (23.6%), with LVH by Sokolow-Lyon voltage in 260 (17.1%) and by Cornell voltage-duration product in 220 (14.6%).
[2] Shah AS, Chin CW, Vassiliou V, et al. Left ventricular hypertrophy with strain and aortic stenosis. Circulation. 2014;130(18):1607-16. (téléchargeable)
Compared with those without left ventricular hypertrophy (n=51) and left ventricular hypertrophy without ECG strain (n=30), patients with ECG strain (n=21) had more severe aortic stenosis
[3] Liang Y, Sau A, Zeidaabadi B, et al Artificial intelligence-enhanced electrocardiography to predict regurgitant valvular heart diseases: an international study. Eur Heart J. 2025 Nov 21;46(44):4823-4837.