
L’hypertrophie biventriculaire cumule des critères d’hypertrophie VG et hypertrophie VD. L’aspect du tracé dépend de la prédominance relative de l’une ou de l’autre. Les anomalies de voltage dues à l’HVG peuvent masquer l’HVD, c’est pourquoi l’ECG manque de sensibilité versus l’échocardiographie [1].
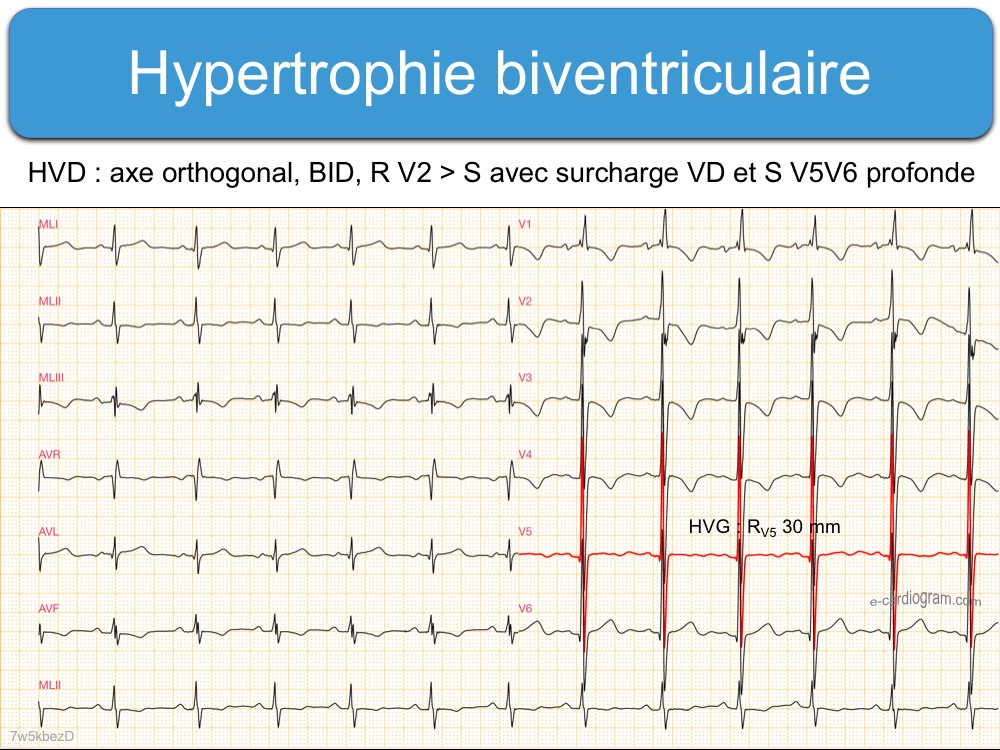
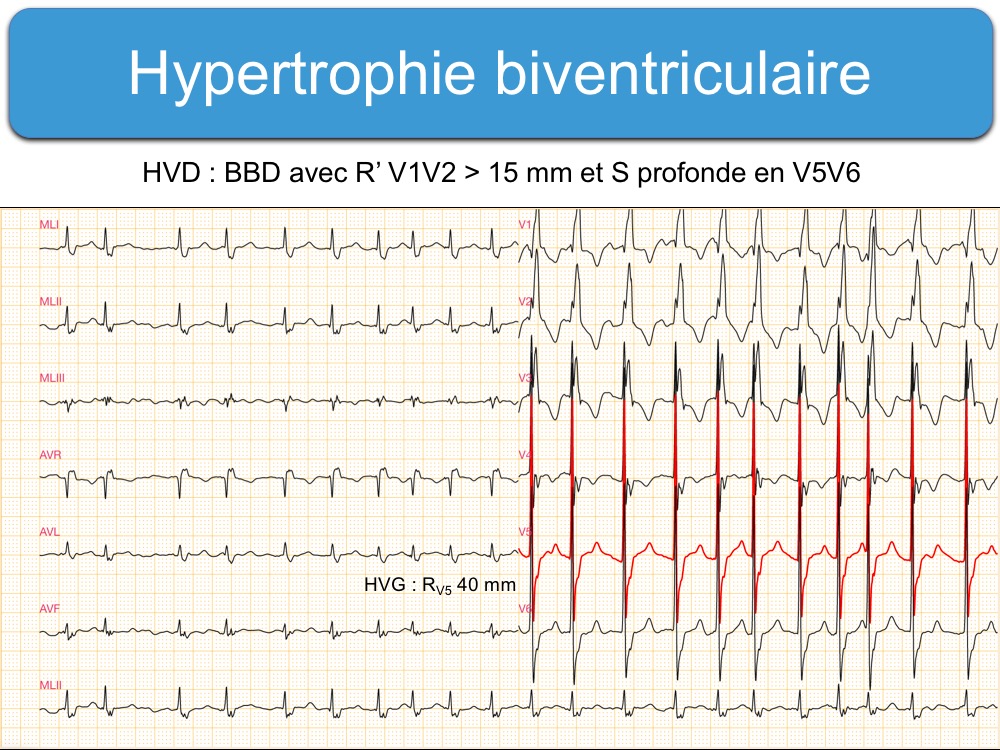
L’aspect évocateur associe un indice d’hypertrophie VG (ex. ondes RV5 ou V6 amples) avec [1] :
- un indice d’hypertrophie VD (onde RV1 > 6 mm avec souvent SV6 profonde),
- ou une déviation axiale droite (ÂQRS > 90°),
- ou des complexes QRS amples dans plusieurs dérivations précordiales combinant des grandes ondes R et des grandes ondes S dont l’amplitude combinée R/S est proche de 50-60 mm (surtout V2-V4),
- des anomalies de repolarisation dans toutes les précordiales de type surcharge ventriculaire.
Hancock EW et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part V: electrocardiogram changes associated with cardiac chamber hypertrophy… J Am Coll Cardiol. 2009;53(11):992-1002. Review. (téléchargeable) –> Right axis deviation in the presence of electrocardiographic LVH and tall biphasic R/S complexes in several leads should be recognized as suggestive of biventricular hypertrophy. –> In patients with congenital heart defects and RVH, the presence of combined tall R waves and deep S waves in leads V 2 to V4 , with combined amplitude greater than 60 mm (6.0 mV), suggests the presence of LVH
Fournier C et Pellerin D. Hypertrophies auriculaires et ventriculaires. Encycl Méd Chir (Elsevier, Paris), Cardiologie-Angéiologie, 11-003-F-50, 1996.