Comment quand anticoaguler (ESC 2024) ?
Les anticoagulants peuvent être utiles pour réduire le risque thromboembolique (TE) associé à une fibrillation ou un flutter atrial [1]. Tous les patients qui présentent une FA doivent avoir une estimation du risque thromboembolique (TE), quel que soit le rythme cardiaque au moment de l’examen (ex. conversion ou cardioversion) [1][2]. L’estimation du risque TE est essentielle à la prise en charge thérapeutique. Elle repose depuis 2024 sur le score CHA2DS2-VA [1].
Lire réf (ESC 2024 [1]).
- Table 6 Recommendations to assess and manage thromboembolic risk in AF
- Table 7 Recommendations for oral anticoagulation in AF
Updated definitions CHA2DS2-VA score ESC 2024 (Table 10)
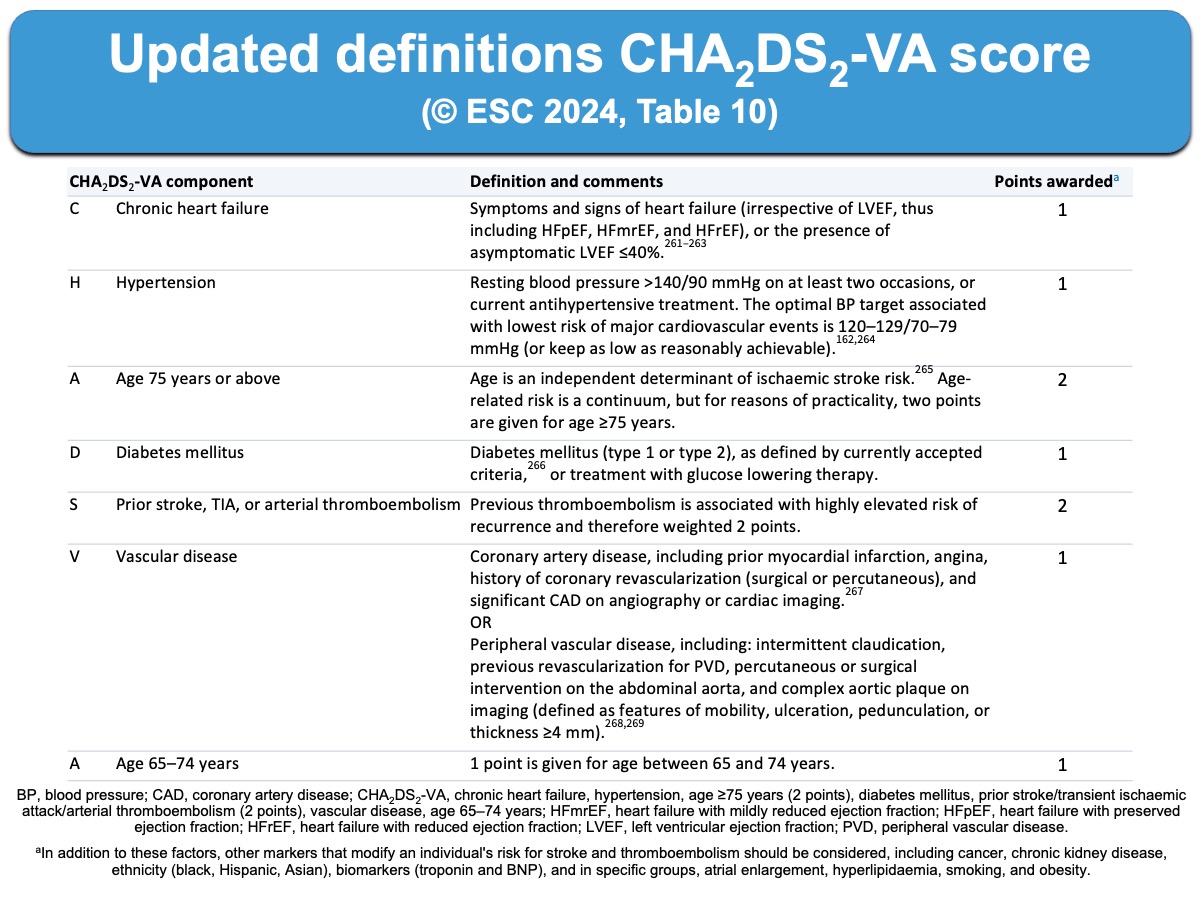
Les facteurs de haut risque d’accident thromboembolique sont : un âge supérieur à 75 ans, un antécédent d’accident vasculaire cérébral (AVC), accident ischémique transitoire (AIT) ou embolie systémique [1], un rétrécissement mitral ou la présence d’une prothèse valvulaire cardiaque mécanique [3].
Un traitement anticoagulant au long court par anticoagulant oral est recommandé en présence d’un seul facteur de risque thrombo-embolique (Classe IIa) et a fortiori ≥ 2 facteurs (Classe I).
Tous les patients présentant une FA doivent avoir une évaluation formelle du risque hémorragique [1]. L’usage d’un score n’est plus recommandé [1].
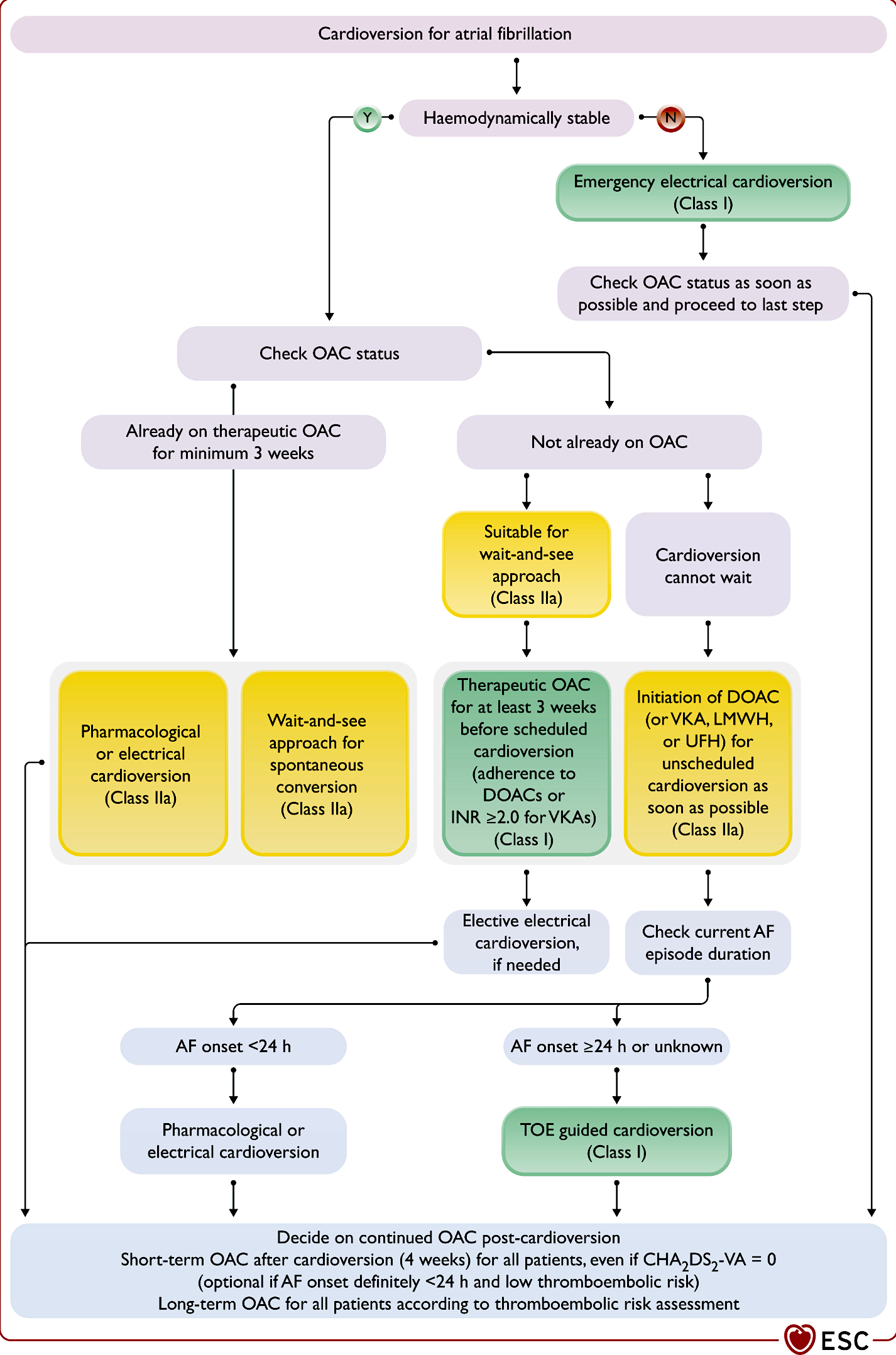
Ue anticoagulation est recommandée en péricardioversion au moins 4 semaines sauf certaines conditions ( cf FA et cardioversion)
ESC 2024, Figure 12. Approaches for cardioversion in patients with atrial fibrillation CHA2DS2-VA.
[1] Van Gelder IC, Rienstra M, Bunting KV,et al; ESC Scientific Document Group. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024 Sep 29;45(36):3314-3414. (téléchargeable)
Hindricks G, Potpara T, Dagres N, et al; ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2020 Aug 29:ehaa612. (free access) Lire aussi Camm AJ, Lip GY, 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC Guidelines for the management of atrial fibrillation. Eur Heart J. 2012;33:2719-47 (free access)
[2] Taboulet P, Duchenne J, Lefort H, et al. Prise en charge de la fibrillation atriale en médecine d’urgence. Recommandations de la SFMU en partenariat avec la SFC. Ann. Fr. Med. Urgence (2015)
[3] Singer DE, et al. American College of Chest Physicians. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):546S-592S.
[4] Pisters R et al. A novel user friendly score (HAS-BLED) to assess one-year risk of major bleeding in atrial fibrillation patients: The Euro Heart Survey. Chest. 2010;138(5):1093-100
La suite est réservée aux membres et stagiaires du site.
Se connecter | Devenir membre | Devenir stagiaire