Erreurs particulièrement fréquentes dans la pose des électrodes précordiales qui génèrent des erreurs d’interprétation et de reproductibilité [1][2][3] :
- faux bloc incomplet droit
- fausse hypertrophie atriale gauche
- faux ST+
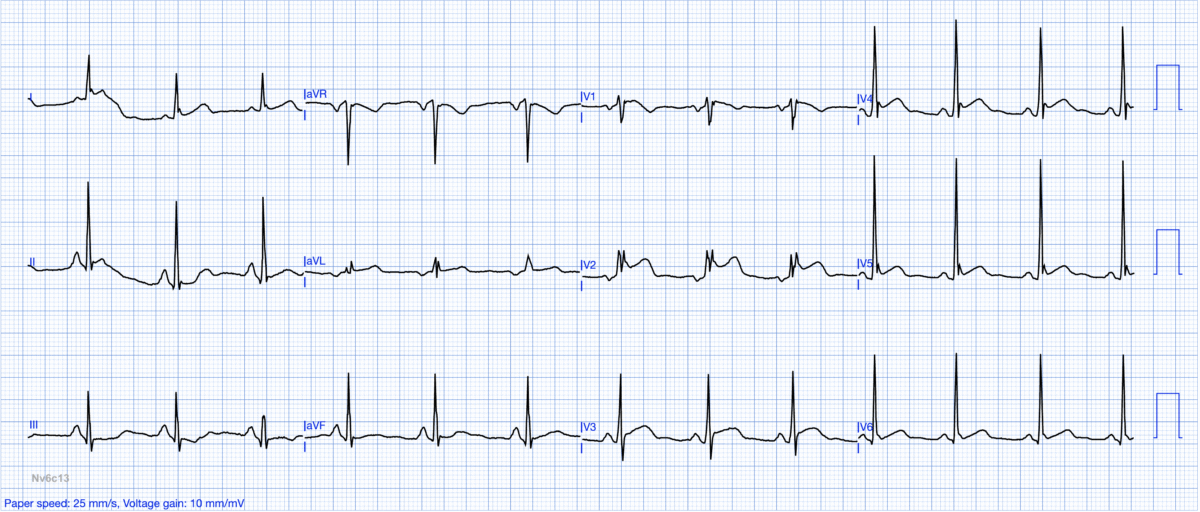
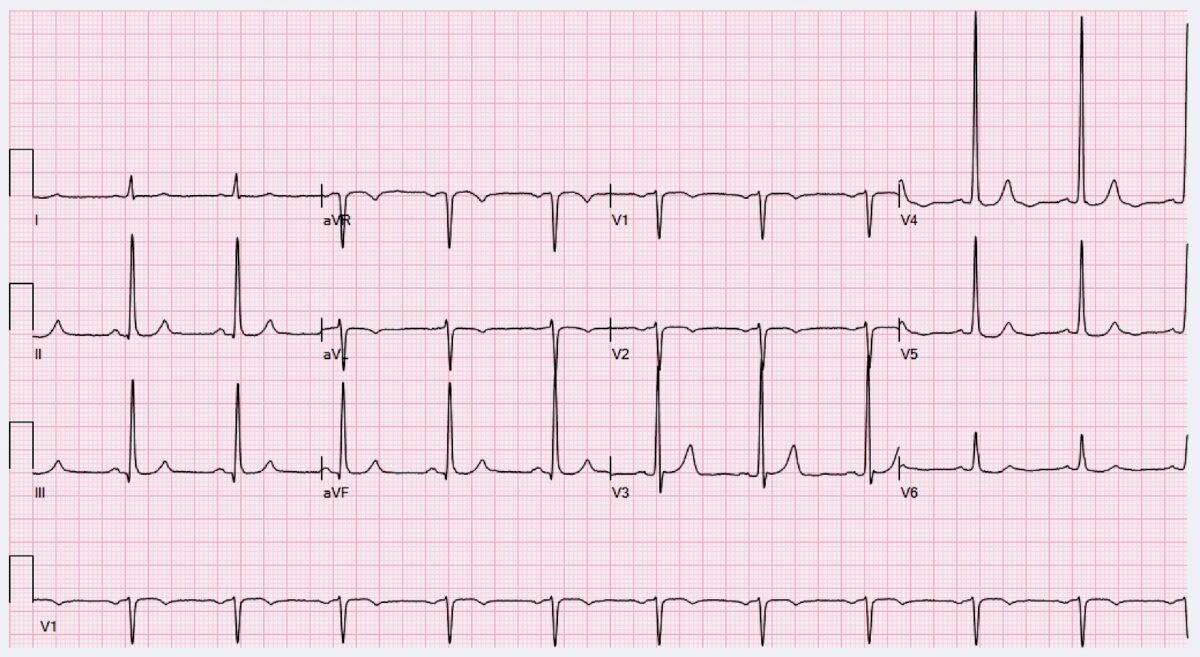
Ci-dessous. V1V2 trop hautes avec pseudo infarctus ST+ du à la repolarisation précoce
- fausse onde Q de nécrose
- faux « Brugada » (aspect du ST-T en selle de cheval)

- microvoltage masquant une HVG
- anomalie de repolarisation (masquée ou ajoutée, ex. T négative en V2)

Vidéo. P. Taboulet. Comment enregistrer un ECG
Vidéo. P. Taboulet. Séquelle d’infarctus septal ?
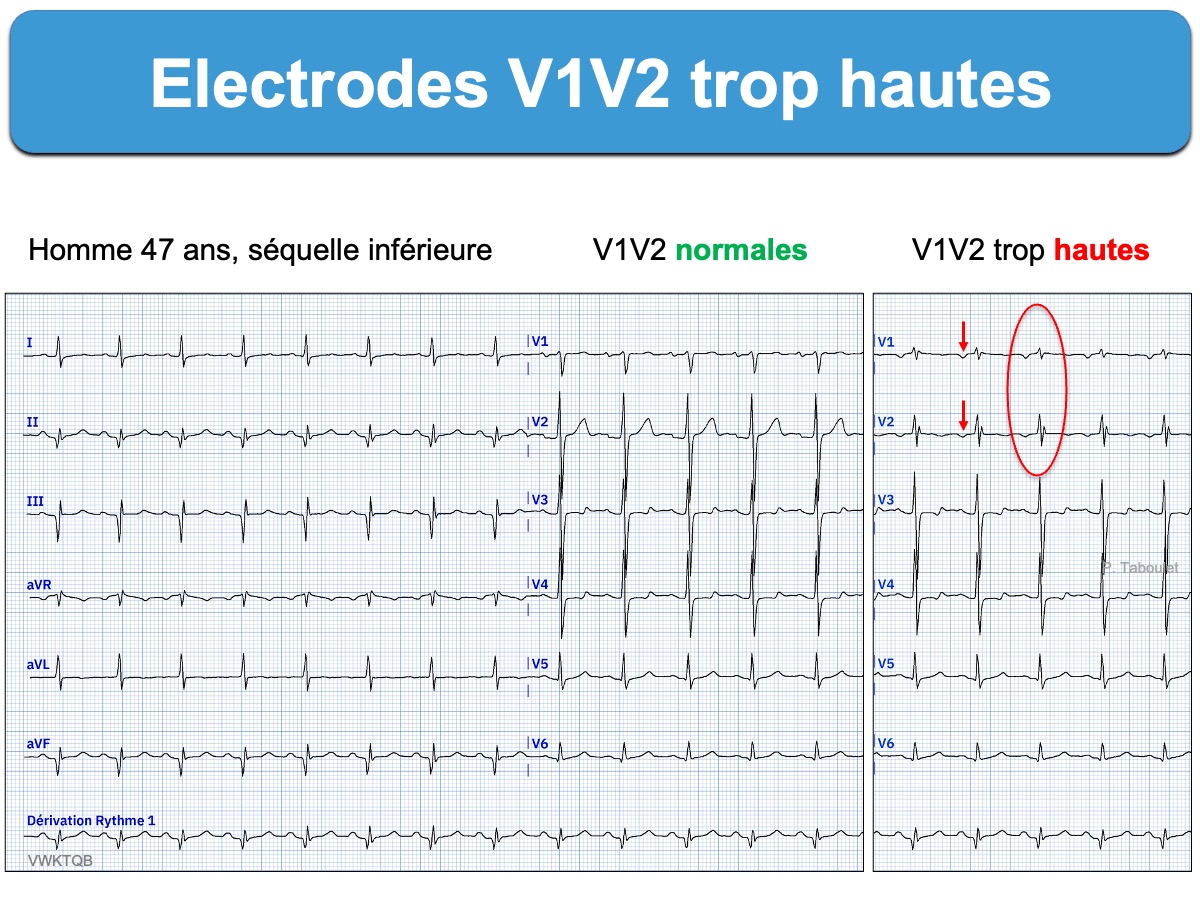
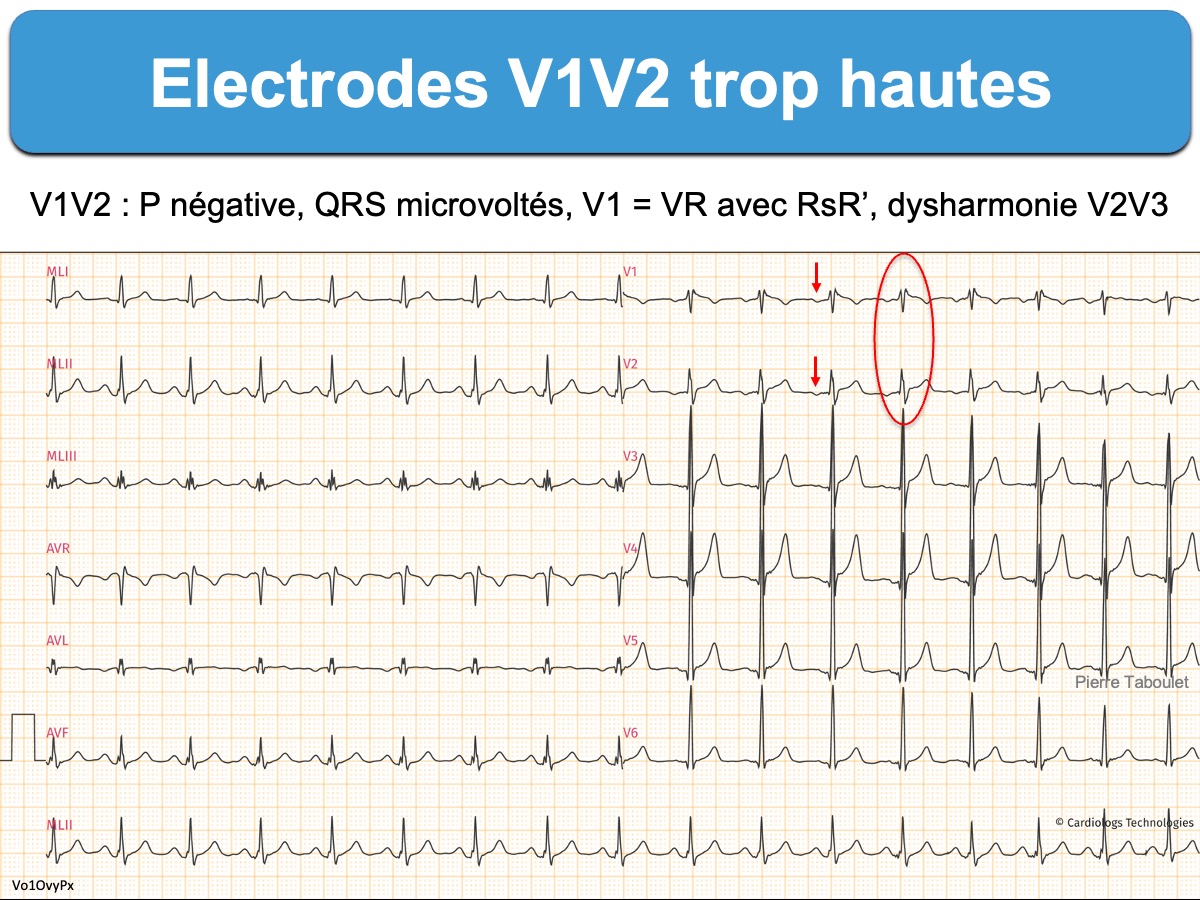
Repérage de V1V2 trop hautes
Anomalies évocatrices en V1V2
- ondes P à prédominance négative en V1 ou V2 ou biphasique en V2 car les oreillettes sont « vues de haut » (LITFL [7])
- onde R’ en V1 ou V2 simulant un bloc incomplet droit
- complexes QRS plus petits qu’en V3V4 (ce qui crée une dysharmonie de V2 à V3) ou aspect QR simulant une séquelle de nécrose [2][4][8]
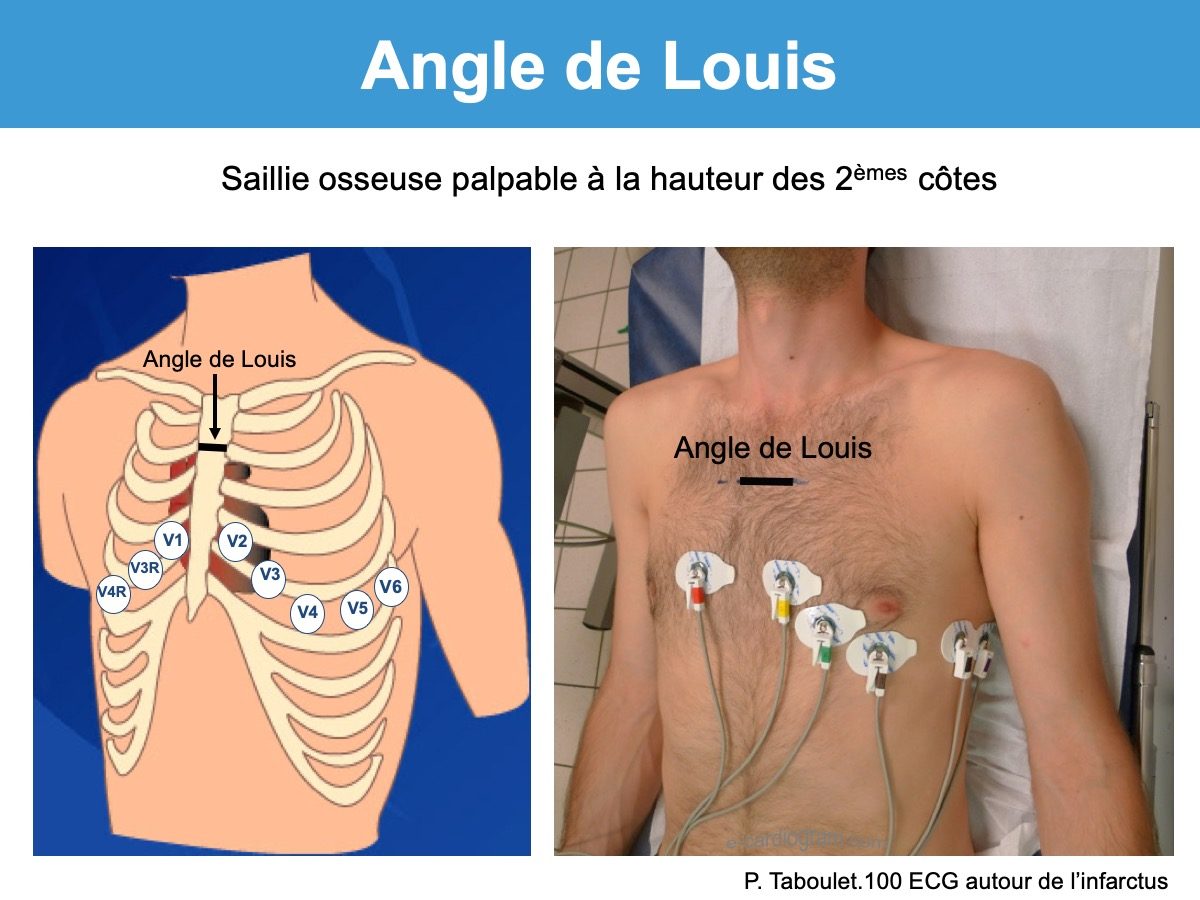
Rappel technique
Il faut poser les électrodes V1-V2 au 4e espace intercostal. Pour cela, il faut :
- repérer l’angle de Louis (qui identifie l’insertion des 2èmes côtes sur le sternum) [5].
- ou (ma méthode [6]) positionner en premier l’électrode V4 dans le sillon sous mammaire gauche sur la ligne médio-claviculaire (fossette palpable avec l’index), puis poser V2 en parasternal gauche, 1 espace intercostal plus haut, puis poser V1 en parasternal droite en regard de V2, puis V3 exactement entre V2 et V4 et on poursuit avec V5 et V6 sur la même ligne que V4 (cf. Électrodes précordiales) [6].
Une aide au repérage du mauvais positionnement des électrodes par les algorithmes d’interprétation ou « machine learning » est possible [2].
Quiz : les électrodes sont-elles bien positionnées ?
Réponse au quiz ci-dessous (abonnés premium)
YouTube : ma playlist
Faîtes des quiz sur le site web (plusieurs niveaux de connaissance 1 à 3).
Ex. quiz technique et pièges niveau 2
Si vous souhaitez améliorer ce contenu, merci de me contacter
Quiz : ECG Brugada type 2 ?

Réponse: Is this Septal STEMI/OMI? Many examples of Septal STEMI/OMI
Références commentées (réservées aux abonnés)
La suite est réservée aux membres et stagiaires du site.
Se connecter | Devenir membre | Devenir stagiaire